
Smart cements for indirect bonded ceramic restorations
October 13, 2025
|
In contemporary restorative dentistry, the use of self-etch adhesives has become a very routine practice. However, there are certain shortcomings of these cements, the most common one being the “clean up” during the cementation process. On occasions, if there is even a slight delay in cleaning the cement, it gets stuck in the interproximal embrasures. This can then be rather difficult to remove.

Fig. 1 – The lower first molar has a failing amalgam restoration and a buccal wall cavity as well. Appropriate isolation is achieved using a rubber dam.

Fig. 2 – The tooth is cleaned using rotary instruments. Selective etching is performed with 37% phosphoric acid (Gel Etchant, Kerr).

Fig. 3 – IDS and the buccal cavity were restored with a flowable bulk-fill restorative material (Simplishade, Kerr) after the application of a universal bonding agent (OptiBond™ Universal, Kerr). A digital impression was taken and sent to the lab for the fabrication of an indirect ceramic restoration.

Fig. 4 – After receiving the prosthesis, the temporary restoration was removed.

Fig. 5 – The indirect restoration, once received and verified for fit, is treated following the appropriate protocol. 9% hydrofluoric acid was applied for 20 seconds and then rinsed off. To remove debris and ensure a properly cleaned surface, the restoration was etched with 37% phosphoric acid for 60 seconds and then rinsed. Silane was then applied with a brush and air-dried.

Fig. 6 – Air abrasion was performed using 27-micron aluminum oxide.

Fig. 7 – Selective etching was done using 37% phosphoric acid (Gel Etchant, Kerr). Ceramic primer was then applied to the exposed composite resin.

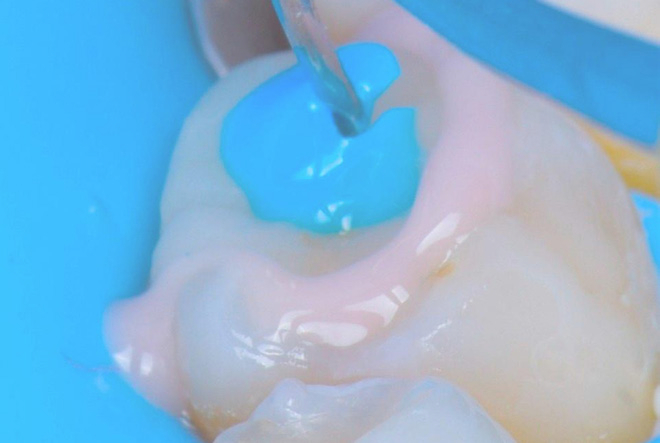
Fig. 8 – A universal bonding agent (OptiBond Universal, Kerr) was applied. Dual-cure cement (Maxcem Elite Chroma™, Kerr) was then extruded into the cavity. At the time of placement, the cement was pink in color.

Fig. 9 – Dual-cure cement (Maxcem Elite Chroma, Kerr) was extruded into the cavity. At the time of placement, the cement appeared pink in color. Through a reduction-oxidation reaction, the pink color of the Maxcem Elite Chroma gel point indicator responds to the polymerization process via its patented redox initiator system, causing the color to fade as curing progresses.

Fig. 10 – The ceramic lithium disilicate restoration was placed on the tooth with the help of an instrument bonded to the ceramic surface using a block-out resin typically used for in-office tooth bleaching. When the dual-cure cement begins to shift to an off-white color, it indicates the appropriate time to clean the excess. This color change serves as a very helpful visual guide during the cleanup phase.

Fig. 11 – After the initial cleanup and cement set, the restoration is covered with a liquid glycerine gel and then polymerized for 40 seconds on each side.

Fig. 12 – The restoration is then given a final luster using an appropriate polishing rubber (Opti1Step; Kerr Co.). This results in a well-integrated indirect restoration with no flash cement remaining in the embrasures.
Conclusion
The use of a color-changing, self-etching cement, in combination with appropriate bonding protocols, facilitates easy cleanup during the cementation process. This is extremely beneficial to the clinician, resulting in a well-integrated restoration with no postoperative sensitivity and contributing to long-term success.
Bibliography
Tosco V, Monterubbianesi R, Orilisi G, Sabbatini S, Conti C, Özcan M, Putignano A, Orsini G. Comparison of two curing protocols during adhesive cementation: can the step luting technique supersede the traditional one? Odontology. 2021 Apr;109(2):433-439.
Koubi S, Raskin A, Dejou J, About I, Tassery H, Camps J, Proust JP. Effect of dual cure composite as dentin substitute on the marginal integrity of Class II open-sandwich restorations. Oper Dent. 2010 Mar-Apr;35(2):165-71.
Blatz MB, Sadan A, Kern M. Resin-ceramic bonding: a review of literature. J Prosthet Dent 2003;89:268-74.
Disclosure: Dr. Ajay Juneja is a consultant for Kerr. The opinions and technique expressed in this article are based on the experience of Dr. Ajay Juneja. Kerr is a medical device manufacturer and does not dispense medical advice. Clinicians should use their own professional judgment in treating their patients. All trademarks and brand names are the property of their respective owners.
MKT-25-0448 Rev-0

Share This







